

New Data Available from DHS-7 Questionnaire: Maternal and Pregnancy-Related Mortality

© 2016 Riccardo Gangale/VectorWorks, Courtesy of Photoshare
In 2014, The DHS Program began the process of updating the standard DHS questionnaires. With input from stakeholders, feedback from in-country implementing agencies, and a host of lessons learned from the previous 5-year program, we added, modified, and, in some cases, deleted questions. For many indicators, the actual questionnaire did not require an adjustment, but the calculation of indicators or the tabulation of the data needed an update to reflect new international indicators and best practices.
While questionnaire revision started in 2014, it can take a long time to see this exercise bear fruit. The 2015-16 Malawi DHS, for example, went into the field with the DHS-7 updated questionnaires in October 2015. The final report and dataset for the 2015-16 Malawi DHS were released in March 2017, allowing us to explore the new data for the first time.
In this blog series, New Data Available from DHS-7 Questionnaire, we will be detailing, topic by topic, some of the key changes to the questionnaire, with a focus on why the changes were made, how the changes affect the tabulations, and some guidance on how the resulting data should be interpreted.
Part 1: Maternal and Pregnancy-Related Mortality
 DHS surveys now collect data to provide the maternal mortality ratio in line with the definition provided by WHO. For almost 30 years, The DHS Program has collected data on maternal mortality in a subset of countries. In previous DHS cycles, maternal mortality was defined as any death to a woman while pregnant, during childbirth, or within two months of delivery. The WHO definition of maternal mortality is more precise: any death to a woman during pregnancy, childbirth, or within 42 days of delivery but not from accidental or incidental causes (see full WHO definition here). The new DHS-7 questionnaire allows us to calculate the maternal mortality ratio (MMR) in closer alignment with this more precise WHO definition.
DHS surveys now collect data to provide the maternal mortality ratio in line with the definition provided by WHO. For almost 30 years, The DHS Program has collected data on maternal mortality in a subset of countries. In previous DHS cycles, maternal mortality was defined as any death to a woman while pregnant, during childbirth, or within two months of delivery. The WHO definition of maternal mortality is more precise: any death to a woman during pregnancy, childbirth, or within 42 days of delivery but not from accidental or incidental causes (see full WHO definition here). The new DHS-7 questionnaire allows us to calculate the maternal mortality ratio (MMR) in closer alignment with this more precise WHO definition.
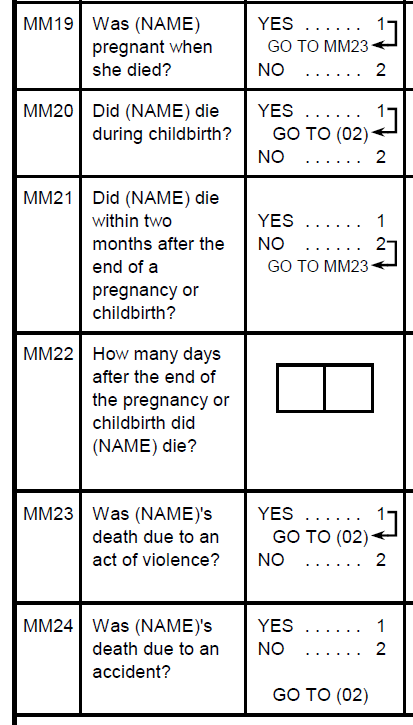
As always, women interviewed in the DHS are asked to list their siblings. The interviewer then collects information about the siblings’ survival status. In the case of female siblings who have died at age 12 or older, the interviewer inquires whether or not the sister died during pregnancy, childbirth, or within the 2 months following delivery. If the sister died within 2 months after childbirth, the interviewer asks how many days after childbirth the sister died. This clarification on the number of days is a new addition to the DHS-7 questionnaire. The interviewer then asks additional questions to determine if the death was accidental or due to violence. In DHS-7 these deaths are excluded from the calculation of the MMR per the WHO definition.
Why? These changes were made to improve the precision of the MMR, as well as to align the DHS estimation of the MMR with the standard definition provided by the WHO.
Implications: While the newly added questions allow for a more precise and up-to-date measure of maternal mortality, the change does present challenges for interpretation. DHS has reported on maternal mortality for 30 years, but estimates obtained using the new definition of maternal mortality cannot be directly compared to the old definition of maternal mortality which included deaths up to 2 months after delivery and did not exclude deaths due to accidents and violence.
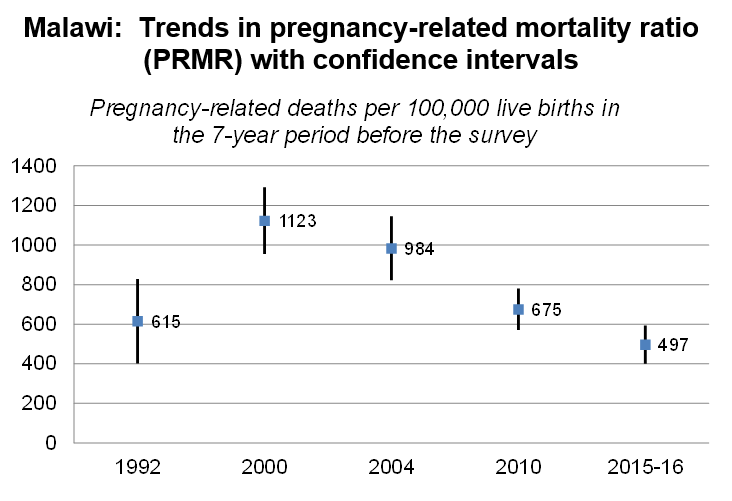 And yet, one of the main objectives for conducting DHS surveys is to provide trend data. Fortunately, the old definition of maternal mortality can still be applied to calculate the mortality ratio estimate comparable to estimates from previously collected mortality data. This less precise measure of mortality is referred to as the pregnancy-related mortality ratio (PRMR).
And yet, one of the main objectives for conducting DHS surveys is to provide trend data. Fortunately, the old definition of maternal mortality can still be applied to calculate the mortality ratio estimate comparable to estimates from previously collected mortality data. This less precise measure of mortality is referred to as the pregnancy-related mortality ratio (PRMR).
DHS reports that include the maternal mortality module will now contain both the maternal mortality ratio and the pregnancy-related mortality ratio. The maternal mortality ratio will be used as the primary point estimate, but the pregnancy-related mortality ratio will be shown in an additional table and in figures to illustrate the trend. Keep in mind that the new measure of maternal mortality, by definition, will result in a lower maternal mortality ratio than the old measure because the accidental and violence-related deaths to women during the maternal period and deaths occurring between 42 days and 2 months after childbirth are being excluded from maternal deaths while using the new definition but included while using the old definition.
Summary of Maternal Mortality and Pregnancy-related Mortality:
| Maternal Mortality Ratio | The number of maternal deaths to any woman during pregnancy, childbirth, or within 42 days of delivery excluding accidents and acts of violence per 100,000 live births | More precise | Not comparable to surveys before DHS-7 |
| Pregnancy-related Mortality Ratio | The number of pregnancy-related deaths (deaths to a woman during pregnancy or delivery or within 2 months of the termination of a pregnancy, from any cause, including accidents or violence per 100,000 live births | Less precise | Comparable to previous surveys; shown to allow for trend interpretation |
The DHS-7 questionnaire includes additional prompts to fully capture more siblings and siblings’ deaths. In previous DHS questionnaires, women were asked to list their siblings in order and then were asked follow-up questions about their survival status. In the DHS-7 adult mortality module, respondents are asked to list their siblings without worrying about their order but are then asked a list of probing questions to ensure that all siblings have actually been recorded. This change is likely to produce a more complete list of siblings for which information on adult and maternal mortality is collected. Once a complete list is produced they are then ordered and the questions on their survival status and age or age at death and years since death, as well as the maternal mortality related questions, are then asked as applicable.
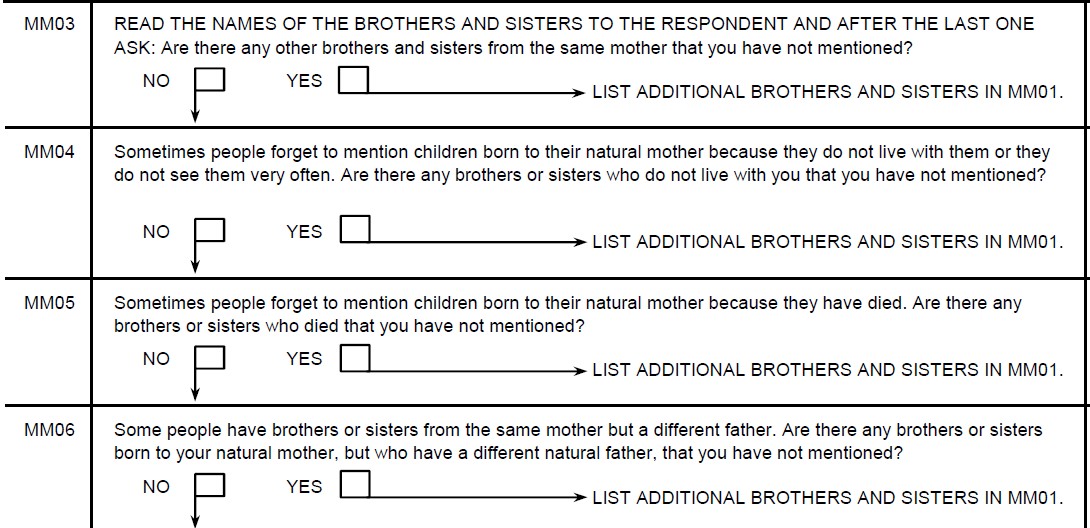
Why? Several studies have suggested that respondents’ lists of siblings are not always complete. This often happens when the sibling is a half-brother or sister, when the sibling did not live with the respondent as a child, or when the sibling has died. A pre-test in Ghana indicated that the addition of these probing questions resulted in capturing additional siblings for about 10% of women.
Implications: Omissions in the sibling history can affect the adult and maternal mortality ratios in different ways. The inclusion of more siblings tends to increase the adult mortality rate. This is because often the siblings who were previously omitted were not spontaneously mentioned because they have already died. However, studies suggest that these deaths are not disproportionately maternal deaths, so a more complete sibling listing might result in a lower maternal mortality ratio.
Key Take-Aways
The changes described above may sound confusing for non-demographers. The major points to remember for DHS data users include:
- The new Maternal Mortality Ratio is not comparable with previous measures of maternal mortality in DHS surveys
- For trends, look at Pregnancy-related Mortality Ratio
- Despite the different names, both measures include deaths during pregnancy. The MMR is a more precise measure as it excludes some of the deaths during pregnancy that were not related to pregnancy (i.e. accidents and acts of violence).
- Maternal mortality is still a relatively rare event, and therefore both MMR and PRMR have wide confidence intervals. Both measures are always presented with their confidence interval so that the user can draw their own conclusions about the relative certainty of the point estimate.
Interesting! As a maternal health expert I am interested to join the Blog.
You can subscribe to our blog posts here and receive alerts when a new blog is posted!
I am interested to join the blog. I am a demographer.
Thank you for your interest Yagya! You can subscribe to our blogs here. You can also subscribe to our newsletter that updates our subscribers on our most recent publications and another DHS news.